Adoption of AI in Healthcare: A Practical Roadmap
Most healthcare leaders no longer need to be convinced that AI matters. They need a clearer answer to a harder question: how do you move from interest to real operational value without getting stuck in a pilot that never scales?
The urgency is real. In 2025, healthcare reached 22% adoption of domain-specific AI tools, a 7x increase from 2024, with health systems at 27% adoption according to Menlo Ventures' 2025 healthcare AI analysis. That shift changes the conversation. The adoption of ai in healthcare is no longer a speculative innovation program. It's becoming part of how organizations protect margins, reduce administrative drag, and support overextended teams.
The problem is that enthusiasm alone doesn't get results. Many healthcare organizations choose the wrong first use case, build around poor data, underestimate workflow friction, or treat a pilot as proof of scale. That's where projects stall.
This guide takes the practical route. It focuses on the operating decisions that separate a contained experiment from a system that clinicians, operations teams, and executives will use.
Table of Contents
- The New Imperative for AI in Healthcare
- Assessing Your Foundational Readiness for AI
- Designing Your AI Solution Blueprint
- From Pilot Program to Validated Solution
- Scaling AI Initiatives and Overcoming the Pilot Trap
- Choosing Your Partnership Model for AI Development
- Frequently Asked Questions on AI in Healthcare
- What is the best first AI use case for a healthcare organization?
- Why do so many healthcare AI pilots fail?
- How should healthcare organizations handle ethics and oversight?
- How do you train staff for AI adoption?
- Can small or under-resourced healthcare organizations adopt AI successfully?
- Is generative AI the same as healthcare AI adoption?
- How do you know when a pilot is ready to scale?
- What should executives ask vendors before buying healthcare AI tools?
The New Imperative for AI in Healthcare
22% of healthcare organizations implemented domain-specific AI tools in 2025, up 7x from 2024, according to Menlo Ventures' 2025 healthcare AI analysis. Health systems led that adoption at 27%. That matters because the pressure behind AI adoption is operational: staffing gaps, rising administrative load, slower cycle times, and tighter margins.

The shift is easy to misread. Many executive teams still frame AI as an innovation program, which usually leads to scattered pilots, weak ownership, and little measurable impact. In practice, the organizations that get value treat AI as an operating model decision. They pick a constrained workflow, assign a business owner, define what changes in the process, and build from there.
That distinction explains why so many healthcare AI efforts stall after an early demo. The common failure point is not model quality alone. It is the gap between a promising pilot and a workflow that people will use under real clinical and administrative pressure.
Why the urgency is operational
The strongest starting points are usually ordinary, high-friction processes. Clinical documentation creates drag for physicians and nurses. Revenue cycle teams spend hours on repetitive exceptions and manual review. Operations and analytics teams still assemble reports from fragmented systems instead of acting on timely data.
These are not glamorous use cases. They are often the right ones.
They have three advantages:
- The pain is already visible: Leaders can point to delays, backlog, burnout, denials, or avoidable manual effort.
- The outcome can be measured: Teams can track turnaround time, throughput, error rates, handoff delays, and labor saved.
- The path to scale is clearer: If a workflow is repeated across sites, departments, or service lines, a successful pilot has room to expand.
Clinical use cases can create major value too, but the bar is higher. Trust, oversight, workflow fit, and patient safety all need tighter design. That does not make them a poor choice. It means leaders should be honest about the implementation burden before calling something ready to scale.
What leaders should change in their thinking
The better question is not whether to adopt AI. The better question is where AI can remove friction in a way the organization can validate, operationalize, and repeat.
I usually ask leadership teams to pressure-test four points before they approve a first initiative:
| Question | Why it matters |
|---|---|
| Which workflow is failing often enough to justify change now? | AI creates value fastest when tied to a costly bottleneck. |
| Who owns the result after launch? | Projects without an operational owner rarely survive beyond pilot. |
| What decision or task changes if the model performs well? | Value comes from changed work, not from a model sitting in a dashboard. |
| Can this use case expand beyond one team or location? | Scale should be considered at the start, not after a pilot struggles. |
This is the shift many high-level guides miss. The adoption of ai in healthcare is no longer about proving that the technology works. It is about building a repeatable path from pilot to validated workflow, then from validated workflow to scaled deployment. If your team needs a practical way to screen opportunities before you commit budget, use this AI readiness checklist for healthcare teams.
Assessing Your Foundational Readiness for AI
A weak AI project usually fails long before development starts. The signals are easy to spot: no single owner, fuzzy business goals, inaccessible data, and quiet resistance from the people expected to use the system.
That matters because most leaders already expect AI to become central. In a recent industry survey, 83% of healthcare and life sciences respondents said AI will revolutionize the sector in the next 3 to 5 years, and 78% planned to increase AI infrastructure budgets according to NVIDIA's 2025 healthcare and life sciences survey. Budget intent is useful, but readiness is what determines whether that spending delivers real advantage or just more pilots.
Strategic fit comes first
Start by testing whether the proposed AI initiative is tied to a top-tier business or clinical problem. If the answer is vague, stop there.
A solid first project usually meets most of these conditions:
- The pain is already expensive or disruptive: Examples include coding delays, intake bottlenecks, documentation burden, or manual chart abstraction.
- The workflow is defined: You can map where the current process starts, who touches it, and where it breaks.
- An operational leader owns the outcome: Not just IT, not just innovation, but the team that lives with the result.
If you need a structured internal audit, a practical AI readiness checklist for enterprise teams can help frame the right conversations before procurement or build decisions start.
Data maturity is less glamorous and more decisive
Healthcare teams often assume they have enough data because they have large systems. That isn't the same as usable data. EHR exports, scanned PDFs, departmental spreadsheets, legacy coding conventions, and inconsistent labeling can sink a project before the model is tested.
Use this short diagnostic:
- Can you identify the source systems? Know where data lives.
- Can you access it consistently? One-time exports aren't enough.
- Can you match records reliably? Broken joins and duplicate entities create downstream errors.
- Can the target workflow tolerate imperfect data? Some operational use cases can. Others cannot.
Practical rule: Don't ask whether your organization has data. Ask whether a frontline team could trust that data in a live workflow next month.
Organizational readiness is often the hidden blocker
Even a technically sound model can fail if the surrounding organization isn't prepared to adopt it. In healthcare, this usually comes down to buy-in, accountability, and skill.
Ask leadership teams to answer these questions plainly:
- Who signs off on model use in the workflow?
- Which clinicians, operators, or managers will test it first?
- How will staff challenge or override outputs?
- What training will users get before launch?
A candid readiness review should also surface resistance early. Sometimes the issue isn't fear of AI itself. It's fear that an already strained team is being asked to absorb one more tool with unclear benefit.
That concern is valid. The strongest implementations reduce work inside the existing workflow. They don't create a parallel process that staff have to remember when they're already overloaded.
Designing Your AI Solution Blueprint
Once a use case is worth pursuing, design choices start to matter more than slide decks. This is the phase where many teams make decisions that look efficient at first and become expensive later.
The blueprint should answer three things clearly: where the model runs, how data moves, and how the system fits regulated healthcare workflows.
Architecture decisions shape later scale
Organizations weigh cloud, hybrid, and on-premise options against security, latency, procurement constraints, and integration effort. There isn't a universal answer. There is only a fit-for-purpose answer.
For example, an AI tool that supports medical coding or patient data extraction may need to pull from multiple document types, process unstructured text, and push results into downstream review queues. That often favors an API-first design with modular services instead of one tightly coupled application.
A useful reference point is this medical record digitization example in healthcare workflows, where the challenge isn't just model performance. It's reliable ingestion, document handling, exception review, and integration into operational systems.
Governance should exist before the first model version
Healthcare leaders sometimes treat governance as something to formalize after the pilot succeeds. That's backwards. If you're dealing with patient data, governance needs to be designed at the start.
Focus on a few essential elements:
- Access controls: Limit who can view raw data, outputs, and audit logs.
- Data lineage: Track where input data originated and how it was transformed.
- Human review points: Define when a person must verify or approve output.
- Model change control: Versioning matters when outputs affect claims, documentation, or care support.
A clean governance model also reduces confusion across legal, compliance, IT, and operations teams. Without it, projects stall in review cycles because no one can explain what the system does in production terms.
Compliance should be built into the design, not layered on top
HIPAA, internal privacy policies, security reviews, and vendor risk assessments don't disappear because the use case is "just a pilot." Teams should assume from day one that any useful pilot may need to scale.
Here's a simple comparison:
| Design choice | Short-term appeal | Long-term risk |
|---|---|---|
| Standalone AI app | Fast to demo | Harder to embed into daily work |
| API-first service | More setup upfront | Easier integration with EHR-adjacent systems |
| Loose file-based handoffs | Simple for early testing | Weak auditability and brittle operations |
| Structured event logging | More engineering effort | Better traceability and governance |
The blueprint should describe how a user acts on an AI output, not just how the model produces one.
A good healthcare AI design feels less like an experiment and more like a controlled extension of the existing operating model.
From Pilot Program to Validated Solution
Most healthcare AI projects don't fail because the first demo is bad. They fail because the pilot proves too little.
The data on this point is blunt. In a survey of healthcare institutions developing or deploying AI use cases, only 19% reported high success in clinical diagnosis AI pilots and 38% reported high success in clinical risk stratification. The same study found that tool uptake was the primary success metric in 74% of cases, and only 30% of pilots scaled to production, largely due to integration and trust barriers according to the published healthcare AI adoption study on PubMed Central.
That changes how a pilot should be run. Accuracy matters, but it isn't enough. A pilot must answer whether people will use the output, whether it fits the workflow, and whether the organization can support it after the test ends.
What a real pilot looks like
Consider a narrow operational use case such as extracting patient information from incoming documents before staff review. The model's job isn't to replace judgment. It's to reduce repetitive handling and speed up the review queue.
A practical implementation pattern looks similar to this automated patient data extraction workflow, where the useful question isn't just 'Did the model parse text?' It's 'Did staff move through work faster without losing confidence in the output?'
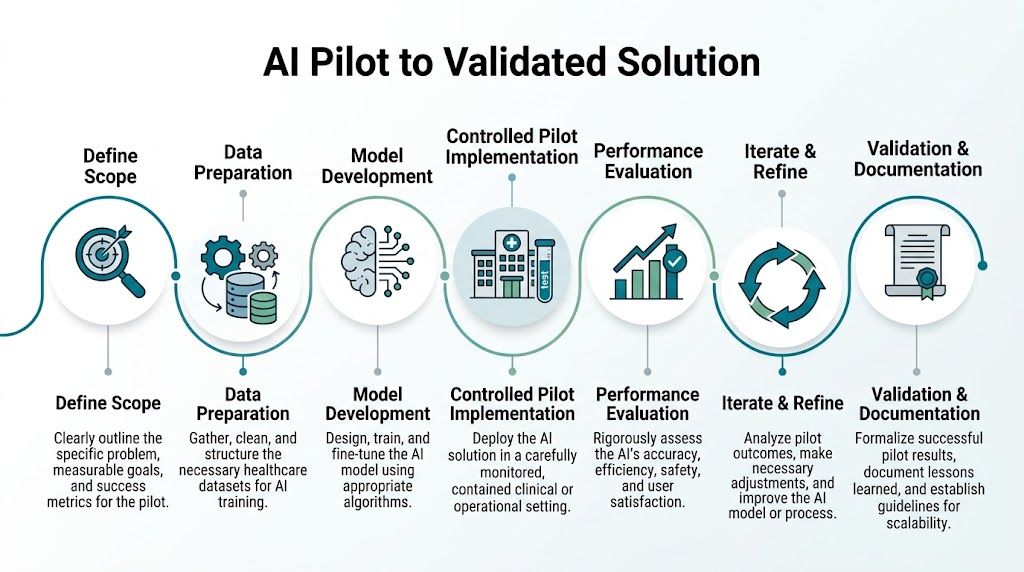
Seven steps that de-risk the pilot
Define a narrow scope
Choose one workflow, one user group, and one operational objective. Broad pilots create muddy evidence.Set success measures before deployment
Include adoption, turnaround time, exception rates, and user confidence. If all you measure is model performance, you'll miss the core decision.Use real data in controlled conditions
Shadow mode is often the safest starting point. Let the system process live inputs without changing production actions yet.Design the review experience carefully
The interface matters. Staff need to see outputs, uncertainties, and what requires verification.Collect structured user feedback
Don't settle for "seems fine." Ask where the system slows work, confuses users, or creates duplicate effort.Compare against the baseline
Teams need evidence that the AI-assisted workflow is better than the current one, not just technically interesting.Document failure modes
A good pilot records edge cases, escalation paths, and conditions where the model shouldn't be trusted.
If clinicians or operations staff can't tell when to rely on the tool and when to override it, the pilot isn't validated yet.
What usually goes wrong
Pilot teams often try to impress steering committees with breadth. They pull in too many departments, too many document types, or too many edge cases too early. That creates noise instead of proof.
Another common failure is weak ownership. If no operational manager is accountable for adoption, the pilot becomes a technology exercise. Users test it politely, then return to the old process.
The pilot stage should feel disciplined, not ambitious. Its job is to earn the right to scale.
Scaling AI Initiatives and Overcoming the Pilot Trap
A pilot can succeed and still be unscalable. That's the part many organizations learn too late.
Industry analysis says 80% of healthcare AI projects fail to scale beyond pilots, often because of data reality gaps and workflow mismatches. The same analysis notes that diagnostic models can drop from 95% lab accuracy to 70% in production when they hit fragmented real-world data, according to this analysis of the healthcare AI implementation gap.

Scaling fails when teams mistake validation for operational readiness
A validated pilot proves that a use case has promise in a bounded setting. Scale demands something else: resilient pipelines, consistent monitoring, reliable handoffs, and organizational adoption outside the original champion group.
Three assumptions usually cause trouble:
- "If the model worked once, it will work everywhere." Different sites, specialties, and data entry habits break that assumption quickly.
- "Users will adapt once value is obvious." They often won't, unless the workflow is redesigned around them.
- "IT can absorb this after launch." Without dedicated operating ownership, support tickets and model drift pile up.
Hardening the system for production
Production healthcare AI needs an operating layer around the model. That's where MLOps becomes practical rather than theoretical.
Core production disciplines include:
| Capability | What it prevents |
|---|---|
| Data pipeline monitoring | Silent failures from missing or malformed inputs |
| Model version control | Confusion about which output came from which model state |
| Drift detection | Slow performance erosion in live settings |
| Fallback workflows | Operational disruption when the AI service is unavailable |
A broader enterprise AI adoption perspective is useful here because scaling rarely breaks on the model alone. It breaks on supportability, governance, and the absence of a repeatable rollout pattern.
Operating principle: Every scaled AI workflow needs a non-AI fallback path that teams can execute without confusion.
Change management is part of the technical rollout
Many executive teams often underinvest. They assume a good product experience will handle adoption. In healthcare, role clarity matters more.
Give each deployment wave named owners across these groups:
- Clinical or operational sponsor: Owns business impact and workflow decisions.
- IT lead: Owns integration, access, and support readiness.
- Compliance and privacy stakeholders: Review controls and escalation pathways.
- Super users: Test the experience in daily work and surface practical friction.
The rollout conversation also needs plain-language guardrails. Staff should know what the system does, what it doesn't do, when they should override it, and who to contact when outputs look wrong.
A short explainer often helps teams align on that production mindset:
Continuous validation is what keeps scale from degrading
The first production deployment isn't the finish line. Real-world healthcare environments change constantly through policy updates, staffing shifts, coding changes, documentation habits, and upstream system changes.
That means governance should continue after go-live. A practical oversight routine usually reviews:
- Model performance in live use
- User adoption and override patterns
- Exceptions and escalation volume
- Workflow impact on downstream teams
The pilot trap isn't just a technical issue. It's an operating model issue. Teams escape it when they treat AI as a managed service inside the business, not a one-time implementation.
Choosing Your Partnership Model for AI Development
Healthcare organizations don't need to build every capability internally. In many cases, they shouldn't.
The right partnership model depends on how much domain expertise, technical capacity, governance maturity, and delivery bandwidth your organization already has. That decision deserves more rigor than the usual build-versus-buy debate.
Not every capability belongs in-house
Some teams should own product and workflow decisions internally while partnering on model development, data engineering, or deployment architecture. Others need a fuller co-development model because their internal team is already stretched across EHR priorities, cybersecurity work, and reporting demands.
Collaborative models can move faster in constrained environments. According to Healthcare IT News coverage of the Health AI Partnership, collaborative consortia like HAIP can accelerate AI adoption 2 to 3 times faster than solo efforts in under-resourced settings. That matters because many healthcare organizations aren't blocked by ambition. They're blocked by time, staffing, and implementation experience.
How to evaluate the model that fits
A simple comparison helps:
| Partnership model | Best fit | Main risk |
|---|---|---|
| In-house build | Strong internal AI, data, and product teams | Slow delivery if healthcare integration skills are thin |
| Specialist consultants | Strategy, audits, or targeted expert input | Knowledge may not transfer into execution |
| Co-development partner | Need to ship while building internal capability | Requires clear governance and ownership |
| Consortium or shared learning network | Resource-constrained organizations | Less control over pace and standardization |
One option in the co-development category is enterprise AI consulting from Amasa Tech, which focuses on AI audits, readiness work, and implementation support. That kind of partner can be useful when a healthcare team wants to keep business ownership in-house but needs external engineering depth and delivery structure.
What to screen for before signing
Don't focus only on model expertise. Ask sharper questions:
- Have they worked with regulated healthcare workflows before?
- Can they integrate into existing systems instead of forcing a greenfield stack?
- How do they handle governance, auditability, and change control?
- What happens after pilot validation?
- Will your internal team be able to operate what gets built?
A weak partner sells a demo. A useful partner explains support, ownership, and production failure modes before contracts are signed.
The strongest AI partnerships reduce execution risk without removing accountability from the healthcare organization itself. That's the right balance. Clinical and operational ownership should remain close to the people who live with the consequences.
Frequently Asked Questions on AI in Healthcare
What is the best first AI use case for a healthcare organization?
Start with a workflow that is repetitive, measurable, and operationally painful. Good candidates often include documentation support, intake processing, patient data extraction, coding assistance, analytics support, or revenue cycle tasks.
Avoid starting with the most sensitive high-stakes clinical use case unless your governance, data quality, and clinical oversight are already mature. Early credibility matters.
Why do so many healthcare AI pilots fail?
They usually fail for practical reasons, not because AI has no value. Common causes include weak workflow fit, poor data usability, unclear ownership, and limited user trust. Pilot teams also tend to over-scope the first deployment and under-design the review process around it.
If the output doesn't fit the actual work of a clinician, analyst, or operations team, the model won't be adopted even if it's technically strong.
How should healthcare organizations handle ethics and oversight?
Responsible adoption needs explicit guardrails. That means defining who can use the system, what data it can access, where human review is mandatory, how overrides are handled, and how errors are escalated.
For many healthcare use cases, AI should support human judgment rather than replace it. Teams should also review outputs for fairness, unintended bias, and the impact on underserved patient groups.
How do you train staff for AI adoption?
The workforce piece is often overlooked. Recent surveys indicate that only 20% to 30% of clinicians report receiving any AI training, as discussed in HIMSS Maryland's review of AI's impact on the healthcare workforce. That gap creates risk because users may either overtrust the system or avoid it entirely.
A practical training approach includes:
- Role-specific instruction: Teach clinicians, operators, reviewers, and managers differently.
- Live workflow examples: Use real scenarios from the target department.
- Override guidance: Show when staff should reject or escalate an output.
- Feedback loops: Give users a clear way to report edge cases and confusion.
Can small or under-resourced healthcare organizations adopt AI successfully?
Yes, but they should stay disciplined. Smaller organizations usually do better when they focus on one narrow workflow, use shared learning where available, and choose implementation models that reduce internal overhead.
Starting with a contained operational use case is often more realistic than launching an enterprise-wide AI program. Clear governance and modest scope beat ambition every time.
Is generative AI the same as healthcare AI adoption?
No. Generative AI is one category inside a broader set of AI capabilities. The adoption of ai in healthcare includes document processing, imaging support, analytics, risk stratification, workflow automation, and decision support, not just chat interfaces or text generation.
Leaders should choose the method that matches the job. Sometimes that's an LLM. Sometimes it's a rules engine, a classifier, an extraction model, or a hybrid system.
How do you know when a pilot is ready to scale?
A pilot is ready when three things are true at once:
- Users adopt it in real workflow conditions
- The organization can monitor and support it operationally
- The process change is clear enough to repeat in new settings
If one of those is missing, scale usually creates more problems than value.
What should executives ask vendors before buying healthcare AI tools?
Ask direct questions about integration, governance, failure handling, and production support.
A short executive checklist:
- How does this fit into our current workflow?
- What data does it require and how is that data governed?
- Where is human review required?
- How do we monitor performance after launch?
- What happens if outputs degrade or the system goes offline?
- Who inside our organization needs to own this day to day?
Those questions usually reveal whether you're looking at a product, a platform component, or a pilot that still needs substantial operational work.
If you're planning your first major healthcare AI initiative, Amasa Tech can help assess readiness, shape the right implementation model, and build production-minded AI workflows that fit real operating environments.